Dr Antoni Chan is a Consultant Rheumatologist and Associate Medical Director at the Royal Berkshire NHS Foundation Trust.
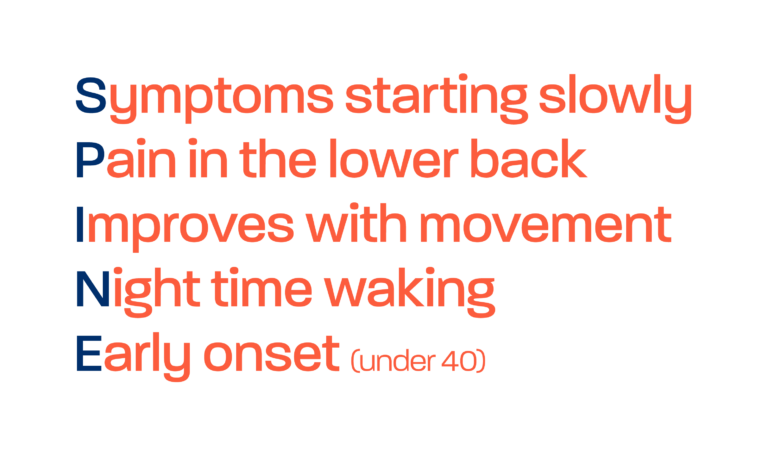
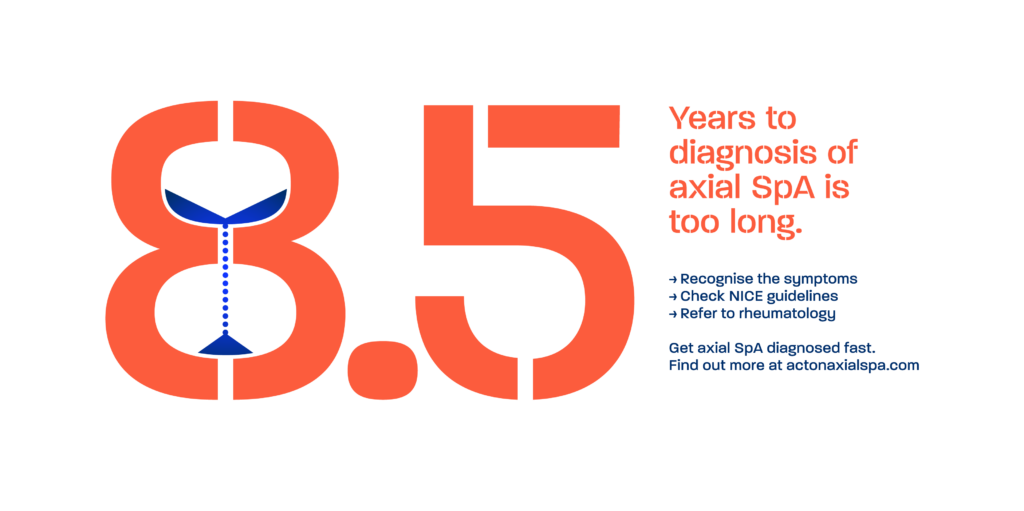
In the UK, it currently takes an average of 8.5 years for a patient to be diagnosed with axial spondyloarthritis (axial SpA). With the Gold Standard time to diagnosis programme, our goal with NASS is to reduce this to just one year. In order to do this, it is critical for us to detect symptoms of axial SpA much earlier on in the condition. In rheumatology, we must be confident in how to further investigate and interpret these symptoms in order to consider a potential diagnosis.
“The main principles of the diagnostic approach can be clearly defined: consider the pre-test probability of the disease, evaluate positive and negative results of the diagnostic test, exclude other entities, and estimate the probability of the disease at the end.”*
*Denis Poddubnyy, Classification vs diagnostic criteria: the challenge of diagnosing axial spondyloarthritis, Rheumatology, Volume 59, Issue Supplement_4, October 2020, Pages iv6–iv17, https://doi.org/10.1093/rheumatology/keaa250